Discussion groups with consumers to consider food safety messaging
As outlined in the methodology, discussion groups were undertaken to explore preferred methods of communicating who the clinically vulnerable groups to foodborne illness are. The in-person discussion groups (n=6) were undertaken in various locations through Scotland with individuals over the age of 65 years and individuals who support people over the age of 65 years (n=50).
Perceptions and preferences of different risk statements among people over the age of 65 years
During the discussion groups, participants were presented with the three different risk statements regarding clinically vulnerable groups to listeriosis. These ranged from the shortest and the least complex statement which was a variation on the standard YOPI categories (Figure 5), an extended YOPI classification which defined specific chronic illnesses and treatments/medication identified in this report that result in reduced immune function (Figure 6) and a statement providing extended YOPI categories specifically defining why the listed groups are clinically vulnerable to foodborne illness which contained the most information (Figure 7). The statements were colour coded and presented to the participants in the ascending order of complexity.
Perceptions and preferences of different risk statements among people over the age of 65 years
The first statement reviewed during the 6 discussion groups was the variation on the standard YOPI categories (Figure 5).
- Some people are more vulnerable to listeria infections, including those over 65 years of age, pregnant individuals and their unborn babies, babies less than one month old and people with weakened immune system.
Figure 5. Pink risk statement (a variation on the standard YOPI categories) presented to the focus group.

Although some participants liked the simplicity of the pink statement (Figure 5), the consensus among the groups was that the statement was “too generic” and did not provide sufficient information. Several participants suggested that the generality of it would result in it being disregarded. This can be illustrated by the comment made by a participant in group 3:
“I feel I would disregard it… I think it’s because it’s so general. There’s so many things that they warn you about, it’s if you’re pregnant, if you’re over 65, and really, I would just look at that and think, “Oh yeah, just another one”.” (Group 3, Respondent 3)
This is consistent with the opinions expressed by the experts during the three panel consultations who concluded that the risk statements that contain only generic information may not be relatable to the clinically vulnerable groups.
Perceptions regarding the extended risk statement
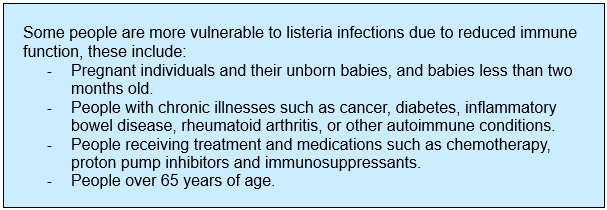
The second statement reviewed during the discussion groups was the extended YOPI classification which defined specific chronic illnesses and treatments, or medication identified in this report that result in reduced immune function (Figure 6):
- Some people are more vulnerable to listeria infections due to reduced immune function, these include:
- Pregnant individuals and their unborn babies, and babies less than two months old.
- People with chronic illnesses such as cancer, diabetes, inflammatory bowel disease, rheumatoid arthritis, or other autoimmune conditions.
- People receiving treatment and medications such as chemotherapy, proton pump inhibitors and immunosuppressants.
- People over 65 years of age.
Figure 6: Blue risk statement (extended YOPI categories defining chronic illnesses and treatments that result in reduced immune function) presented to the focus group.
In comparison to the pink statement (Figure 5), the blue statement was more widely discussed. Many preferred the inclusion of specific conditions and medications that result in reduced immune function. Some suggested that this would catch their attention as is refers to specific conditions.
"I would take far more attention of this because it mentions several things that are important to me. I’m on immunosuppressants. So, there are things there that trigger me so I would immediately read that with more interest and take more consideration of it.” (Group 3, Respondent 5).
“And the list of all of the people who can be affected, detailed list, because I don’t think I would have associated diabetes when I read the first one and I have a friend with diabetes, and I definitely didn’t know that.” (Group 4, Respondent 5)."
However, several individuals suggested that they may not take notice and did not perceive themselves to be vulnerable, even though they had underlying conditions listed in the risk statement. This was often accompanied by the false sense of acquired immunity, or perceptions of invulnerability and optimistic bias. As previously discussed, such perceptions may undermine food safety messaging (Evans & Redmond, 2019) and future messaging needs to combat such perceptions.
“Well, I’ve got diabetes Type 2, but it doesn’t worry me… Well, if you’ve eaten in some of the places in the world, I’ve eaten you become immune to these sorts of things.” (Group 1, Respondent 5).
“I’m over 65. And I think you think, “Well I’m careful so it won’t happen to me. I wash my hands; I look after my food.” And that may be why, I don’t know, people over 65 maybe are more susceptible, like living on their own, having foods that have maybe got out of date because they can’t afford to, you know, buy things frequently or just because they don’t eat it fast enough. I don’t know if that’s what makes people over 65 more vulnerable.” (Group 3, Respondent 4).
“Well, I tick a lot of those boxes. I didn’t realise that. Does it make me think that I am more susceptible? Well, I’m going to say no to that” (Group 5, Respondent 3).
“…if somebody who’s diabetic, that’s a healthy diabetic, would read it and think, that’s rubbish I’m diabetic, I’m fine, so it’s not that easy. I know it’s not that easy, but I think that has to be addressed somewhere” (Group 6, Respondent 3).
Although some participants acknowledged the need for more information regarding clinically vulnerable groups, they were concerned that the level of information in the blue statement would prevent people from engaging with it:
“The blue statement tells it like it is. I find that that pink one is basically sugar-coating things, isn’t it, and people need to know this... I think between the two statements, one is shorter and easier to read, who is going to take the time to read the whole of the blue. So, it’s, there’s more information in the blue but many people get that, they won’t get past the first paragraph, and they will just go hmm and wander off.” (Group 5, Respondent 5).
It was concluded that although the blue statement provided more information about who’s vulnerable, it did not make individuals over the age of 65 years, with listed underlying conditions believe that they were susceptible to foodborne illness.
“It’s obviously got a lot more information there. I still don’t feel vulnerable.” (Group 6, Respondent 1).
“Doesn’t make me feel more vulnerable either.” (Group 6, Respondent 2).
Perceptions regarding the descriptive risk statement
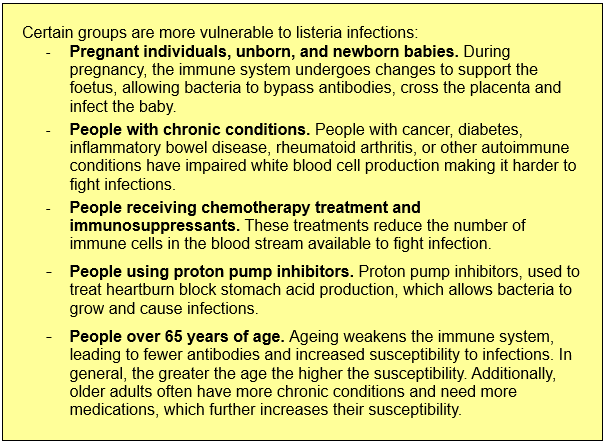
The final risk statement that was discussed during the six discussion groups provided an the extended YOPI categories which specifically defined why the listed groups are clinically vulnerable to foodborne illness (Figure 7):
- Certain groups are more vulnerable to listeria infections:
- Pregnant individuals, unborn, and newborn babies. During pregnancy, the immune system undergoes changes to support the foetus, allowing bacteria to bypass antibodies, cross the placenta and infect the baby.
- People with chronic conditions. People with cancer, diabetes, inflammatory bowel disease, rheumatoid arthritis, or other autoimmune conditions have impaired white blood cell production making it harder to fight infections.
- People receiving chemotherapy treatment and immunosuppressants. These treatments reduce the number of immune cells in the blood stream available to fight infection.
- People using proton pump inhibitors. Proton pump inhibitors, used to treat heartburn block stomach acid production, which allows bacteria to grow and cause infections.
- People over 65 years of age. Ageing weakens the immune system, leading to fewer antibodies and increased susceptibility to infections. In general, the greater the age the higher the susceptibility. Additionally, older adults often have more chronic conditions and need more medications, which further increases their susceptibility.
Figure 7: Yellow risk statement (Extended YOPI categories defining why the listed groups are clinically vulnerable) presented to the focus group.
Although some believed the description to be too long, others felt it to be important and informative. It was discussed that the visual presentation of the information (bold and bullet pointing) made the statement accessible and allowed for a quicker summary by the individuals who felt that the statement was too long:
“Sorry, I fell asleep. It’s far too long.” (Group 2, Respondent 3).
“I find it very interesting actually, very informative. What you’re saying is all these conditions have impaired white blood cell production, which I just find interesting finding out things like that.” (Group 3, Respondent 4).
“I think it very much depends on the communication. I like the blue one because it’s quick and easy but it’s still comprehensive, and there is lots of things in it that I can go and look up. The yellow one is obviously much better but it’s longer and people do tend to have very short attention spans these days. So, you might not read it and then not go and investigate.” (Group 3, Respondent 5).
“It’s comprehensive, isn’t it but you can pick it, it’s got the highlighted bits.” (Group 5, Respondent 3).
“So, you can look at the bullet points and say well, that doesn’t affect me, that would affect me… and then you don’t waste time reading all the bits that you don’t need, you know, and you just go straight to the one that you do.” (Group 5, Respondent 6).
“I like it because it explains why these people are vulnerable.” (Group 2, Respondent unknown).
Many of the participants expressed that they have related to the statement and were surprised to learn that they were at an increased risk of foodborne illness.
“So that’s new to me, a person over 65... I didn’t know that.” (Group 2, Respondent 4).
“I didn’t know that. I knew that pregnant had to avoid soft cheese and all that sort of stuff because of listeria but I didn’t realise that people over 65 were more susceptible.” (Group 4, Respondent 5).
“I fit three of those, and my husband and I between us fit four of those. I’m not pregnant. It’s the only one I’m excused from [laughter], but we fit four of those. Now whilst I know that he is more vulnerable, I’ve always assumed he’s vulnerable because he’s got cancer and he’s having ongoing treatment. I’ve never ever applied that to me, and I’ve got three things there that applies that to me. So perhaps I ought… I think information is power. If you don’t know something, you can never choose to take steps whereas if you do know something, you could either – react by ignoring it or you can act… you have a choice. Yes, you have a choice about how you deal with the situation, and I think, always think, knowledge is power. It does have a scary side, no question but that’s just what it is.” (Group 5, Respondent 3).
“I have never thought I was vulnerable, but I think as you get older, you don’t really want to think you’re getting older. You still think you’ve still got that same constitution as you had when you were young but it will make me … because I’m a wee bit, let’s say, you know, I’m a bit kind of slapdash with things, that is, like, keeping temperature but it will make me think about it more carefully in future and I think that’s education, and I’m quite aware of the connection” (Group 5, Respondent 6).
Many believed that the yellow and blue statements could be used depending on the audience and situation. Nevertheless, one participant did not believe the statements to be educational, with others disagreeing with the statement suggesting that the statement was educational and necessary:
“Unfortunately, all I can see is that you’re going to scare people. Whatever you want to do, its scaring people, they’re just going to go, what?” (Group 5, Respondent 7).
“It’s the education that’s necessary.” (Group 5, Respondent 6).
Awareness of susceptibility to foodborne illnesses
During the discussion groups, participants were asked about the susceptibility to foodborne infection and their immune systems. Many identified pregnant women and people receiving chemotherapy as being clinically vulnerable, however other groups were seldom acknowledged, many had not previously considered themselves as being susceptible and indicated that they weren’t aware that the immune system changes with age:
“When you get older, your system doesn’t have the ability to fight illness as well as it used to. Not at the end of our 50’s, over 60, 65, 70, kind of just your body just… like cars aren’t made to last 70, 80, 90 years, our bodies start to run down and their ability to fight, our immune system isn’t … no matter how well you eat, your immune system is not as rigorous as it was in your 20’s and 30’s.” (Group 2, Respondent 2).
“I find that quite worrying, the new data statistic. I’ve never considered myself high risk. Well, maybe I am, I’ve just turned 70 so maybe I’m high risk.” (Group 2, Respondent 8).
“I wasn’t consciously aware that your immune system declines with age. I know your whole body begins to collapse and different things, but I wasn’t particularly aware that the immune system specifically tended to decline with age.” (Group 3, Respondent 4).
“I think, to be honest, the immune system is something we really don’t think about at all. Unless you have something specific. But, you know, for most people they’ll think of flus and colds and cuts and bruises but the last thing they’ll think about is the immune system. What surprised me with my learning is just how much our health is affected by our immune system. You know, I never knew that arthritis was an immune system thing, you know, until I got it. So, I think people are very unaware of what the immune system actually is or does.” (Group 3, Respondent 5).
“Yeah, cos you’re getting older and it’s not just your immune system, your whole body is reducing to fight you know, it’s been fighting for in my case, 67 years, it’s been fighting and that’s a long time. So (referring to an illness when younger) for one day or two, it’s now three or four or more, so your immune system is tired, worn out.” (Group 4, Respondent 10).
“I suppose the older you get you’re more vulnerable to everything so it’s just one of those things, I guess. It’s not something I’ve really thought about… To be honest I don’t feel vulnerable yet but then, yeah, first time I was aware of things when I was pregnant and things I would obviously be much more careful than... and with the grandchildren when they’ve been tiny, you’re obviously very careful. But I don’t feel vulnerable myself but whether that’s because you don’t like to admit that you’re getting older and of that generation, I don’t know.” (Group 6, Respondent 1).
Appropriate terminology
During the discussion groups, many discussed the appropriate terminology to refer to people over the age of 65. Regarding the term “older adult”, some didn’t have an opinion on the term, whereas others felt that it wasn’t specific enough to identify the clinically vulnerable group. Many indicated that it was important the term used wasn’t patronising, in general people were happy with specifically referring to age.
“But ‘older adults’ is not specific enough. You’ve said, ‘Over 65’, why are we older adults? To be a 50-year-old is probably an older adult really.” (Group 1, Respondent 2).
“Older adults - somebody that’s older than yourself.” (Group 1, Respondent 5).
“My mum was 93 when she died, but she wasn’t old.” (Group 1, Respondent 4).
“If that’s what you’re including, people over 65, then it can say ‘People over 65’.” (Group 1, Respondent 2).
“And ‘pensioners’, people are getting their pensions at all different times now so you can’t say ‘pensioners’ because somebody may not have it yet or may not get it until they’re 70, so I think the 65 is fine.” (Group 4, Respondent 2).
“It’s difficult. It’s an arbitrary number 65. Because there’s old, old 50-year-olds and there’s really young 90-year-olds. So, it’s where the individual fits.” (Group 5, Respondent 4).
“I don’t want a patronising term. Drives me up the wall ‘Elderly’. ‘Older people’, well, how old? I mean, some people think they’re old and they’re 40. How do you define it? That’s a proper category (referring to people over 65).” (Group 5, Respondent 3).
The participants acknowledged that it is important to recognise the differences among people over the age of 65, particularly the presence of other underlying conditions:
“Because if you’re over 65, you know in your own life that you can’t quite do what you used to do necessarily. You know that things have changed but if you don’t have any other condition, then so what, I’m over 65. That doesn’t speak to me. And I actually don’t like it, as if all older people are the same. We’re not all the same.” (Group 2, Respondent 7).
With regards to clinically vulnerable groups, discussion regarding the use of appropriate terminology extended to the use of appropriate imagery to represent people over the age of 65. Indeed, a previous study with people receiving chemotherapy treatment has reported that pictures intended to exemplify people with cancer or receiving chemotherapy were particularly disliked by focus group participants because they wanted to relate to the images (Evans & Redmond, 2022).
“I think the image of older people has changed a lot anyway. So, to come to that point about what are you going to represent older people with, you know, people with sticks or whatever, I think we have aged as a society much more kindly than we did fifty or sixty years ago. So, I think that image of how you’re going to represent older people has to reflect that.” (Group 1, Respondent 3).
“The problem… Well, like we’ve been saying we all feel, you know, reasonably good for our ages, so if you put an 80-year-old up there doddering about and saying, “Be careful about your immune system,” you’d probably think, “That’s not me.” Whereas if you see someone like yourself… Because she looks great (referring to another participant) … And you think, “My gosh, my immune system – I am also vulnerable.” I think that would have more of an impact.” (Group 3, Respondent 3).
“It’s not a flippant thing, it’s quite a serious issue. So yes, I think if you’re going to put photos and stuff in, they need to be relevant.” (Group 5, Respondent 3)
Discussions also considered the opportunity for visual aids to enable people to recognise that they may be at an increased risk of foodborne illness due to age, medication or underlying condition.
Trusted sources of information
The discussion groups also considered who would be trusted sources disseminating information regarding clinically vulnerable groups. Although there was some mistrust regarding the UK government, government departments such as Food Standards Scotland and the UK Food Standards Agency were generally trusted.
“I certainly wouldn’t trust the British Government because they don’t know their arse from their elbow.” (Group 1, Respondent 5).
“And I would probably trust the Food Agency." (Group 5, Respondent 3).
Five of the six groups indicated that the National Health Service (NHS) would be a trusted source of information, however a few participants in one discussion group believed that the NHS was not the most trusted source of information, this was due to the publication of the infected blood inquiry report the week prior to the discussion group (Infected Blood Inquiry, 2024). Although the NHS was trusted overall, some felt that specific healthcare professionals were best placed as trusted advocates for communicating such information such as pharmacists.
“I would to a certain extent trust the NHS.” (Group 1, Respondent 5).
“I would think the medical profession.” (Group 2, Respondent 8).
“Unfortunately, you can’t have the NHS doing it because of the inquiry that’s just going on… That they lied and lied and lied and lied and lied. You can’t have somebody sitting there saying, I’m from the NHS, I’m not decrying the NHS, but you can’t have somebody saying, I’m from the NHS and I’m telling you, that’s what they did to the blood scandal” (Group 5, Respondent 7).
“Yes. I think quite often pharmacists will say to people, you know, “Why are you taking this?” or “Why have you been given this?” They’ve not got quite the same stake in it as the person who’s prescribing it, you know? And they know a lot about how drugs interact and that sort of thing.” (Group 3, Respondent 4).
“I think the pharmacists have become since COVID so much more the first port of call for people that are unwell.” (Group 3, Respondent 3).
Charities that support individuals with specific underlying conditions such as Cancer Research UK and Diabetes UK, were discussed as being trusted sources of information, particularly if they partnered with Food Standards Scotland or Food Standards Agency to communicate the risk of foodborne illness. Similarly, organisations that support people over the age of 65 would be trusted sources of information such as Age UK, Scottish Men's Sheds Association, University of the Third Age, and Scottish Women's Rural Institutes.
Many participants indicated that they would be comfortable with accessing information online, but acknowledged the importance of source checking due to misinformation and conspiracy theorists:
“I’m very sceptical about what’s on the internet because you have to check the source somehow and most of us don’t. So, it needs to be on the internet because that’s the go-to, but it needs to be from a validated place, but I think television advertising, because most people have the television on, not everybody, but most people have it on, so it’s sort of campaign on the television maybe.” (Group 5, Respondent 3).
“You’ve lots of American conspiracy theories with all kinds of nonsense.” (Group 3, Respondent 4).
“I think more and more people are going to be ignoring social media; it’s so packed with crap. Sorry, excuse my language.” (Group 3, Respondent 5).
Summary of discussion groups
Although the participants in the discussion groups were recruited as they were over the age of 65, many identified as belonging to some of the clinically vulnerable groups such as having diabetes, using a PPI or having rheumatoid arthritis. During the discussions, pregnant individuals were particularly identified as being clinically vulnerable to foodborne illness. Participants were generally unaware that they may be at an increased risk of foodborne illness due to age or underlying conditions, nevertheless, many were able to comprehend immune system modifications when given a rationale. Discussions indicated the need to enable people to self-identify if they are at increased risk of foodborne illness. Some people found it easier to accept vulnerability resulting from a medical conditions or medications, rather than age alone. Denial about ageing was also discussed.
Many trusted sources of information were discussed, there are many opportunities for Food Standards Scotland to collaborate with NHS health professionals and other organisations and charities that provide advice, support or services for specific clinically vulnerable groups.
Although these discussions provide insight into potential approaches to communicating who are the clinically vulnerable groups, there is also a need to obtain a deeper understanding regarding the factors that may result in people disregarding food safety messaging. Consequently, exploration of the SEFARI fellowship group discussions with people over the age of 65 and those who support them (n=130) will develop a Holistic Food Safety Behavioural Framework based on potential determinants of food safety risks, behaviours and vulnerabilities, (namely biological, physical, psychological, economic, and social dimensions) along with the constructs of the Health Belief Model (which considers perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy) (Rosenstock, 1974). This will allow an in-depth exploration of the factors that influence food safety behaviours and obtain a better understanding of why food safety messaging may be discarded to refine food safety communication strategies.